
Microscope Hacks
Tips and tricks to up your cytology game


Dear Readers,
Do you have a love/hate relationship with your microscope? Do you dread having to fight with it to focus? Do you struggle to know if what you are looking at is diagnostic or not? I hear these concerns from vets, techs, and nurses all the time, so I wanted to take a moment today to show you a few simple microscopy “life hacks” that should make your cytology experience a lot more diagnostic (and enjoyable)!
Tip #1: Optimize staining
The right staining—not to be confused with WRIGHT staining!—is critical to correctly interpreting samples under the microscope. You want to make sure you have optimized the protocol, understand the pros and cons of each stain, and use best practices to keep them clean.
First off, most vets outside of reference labs will be using Diff-Quik type stains. When we refer to “Diff-Quik,” usually we don’t mean any one single brand, but rather shorthand for any rapid, aqueous Romanowsky-type stain, similar to how “Kleenex” became the universal term for any facial tissues. The upshot is that there are many stain kits out there from different companies with slightly different chemical composition and recommended protocols. In general, the components of Diff-Quik are:

I always recommend starting with the instructions your manufacturer suggests and working from there. Here are some common protocols:
60 seconds in step 1 → 30 seconds in step 2 → 30 seconds in step 3
10 slow dunks in each step
If you have a fatty or mucoid lesion, which are prone to wash off slides and/or have trouble staining, you can leave the slides in fixative longer (DON’T heat fix! It kills cells and makes them uninterpretable). If your stain comes out too light, you can repeat steps 2 and 3 with more dips/longer incubation to enhance staining. Alternatively, if it is too dark to read anything, you can throw it in step 1 and start over—the methanol both fixes and removes stain. Lastly, I don’t recommend rinsing your slide between steps; simply do a light rinse with water (ideally distilled) after completing Step 3. Let it air dry without blotting; you can use a fan without heat to speed the process up.
In contrast to Diff-Quik, which is a water-based stain (methanol is only used in Step 1 as a fixative), the eosinophilic and basophilic dyes for Wright-Giemsa and May-Grunwald-Giemsa use methanol and glycerol as solvents (there are a few other chemical differences), which can change the appearance of slides like so:

The image above shows a few things. First, it provides an example of under-staining that is less ideal for interpretation. Second, it highlights one of the main pitfalls of Diff-Quik: it can fail to stain mast cell granules. As such, you have to be careful not to write off the possibility of a mast cell tumor when you see a population of suspicious round cells without granules on Diff Quik.
Finally, it is important to change your stains often! Precipitate can develop with stain that has been sitting around too long, and microrganisms can grow in them 🤢🤮 Change your stain jars every 1-2 weeks and keep them tightly sealed to the air when not using. You can also minimize contamination by having separate jars of Diff-Quik for gross ear/skin cytology compared to blood smears or FNA cytology.

Tip #2: Know where to look on a slide
You could argue the art of cytology is as much about knowing where to look and what to ignore as actually knowing what all of the lesions are, especially if you are taking pictures and sending them to a remote pathologist for consultation.
First, let’s focus on cell preservation and spreading, and where the optimal places on a slide are to evaluate. Nothing is worse than getting a high cellularity sample, but looking in the wrong places! This diagram shows a schematic view of what I look for in each part of a smear and the pros/cons.
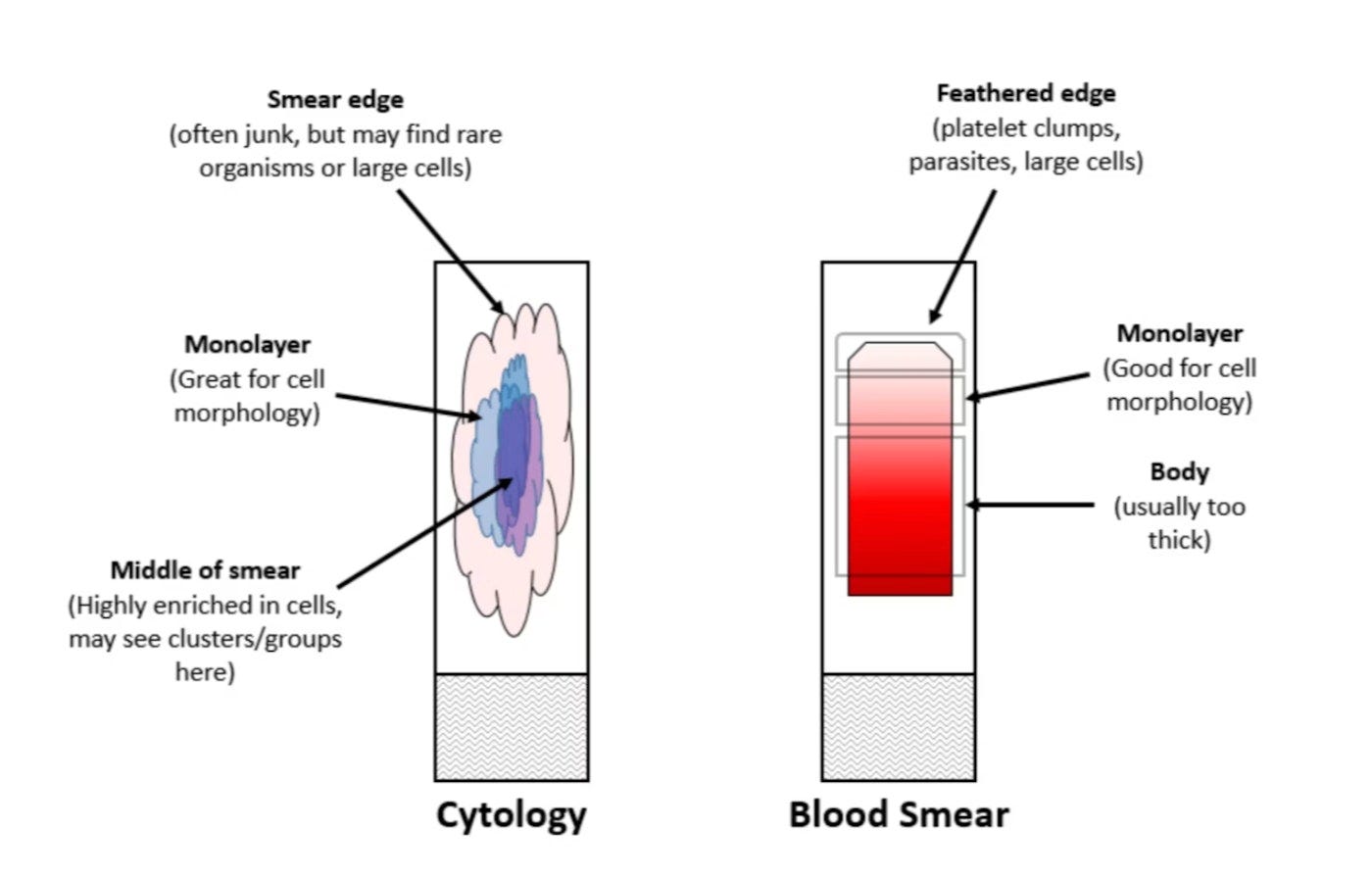
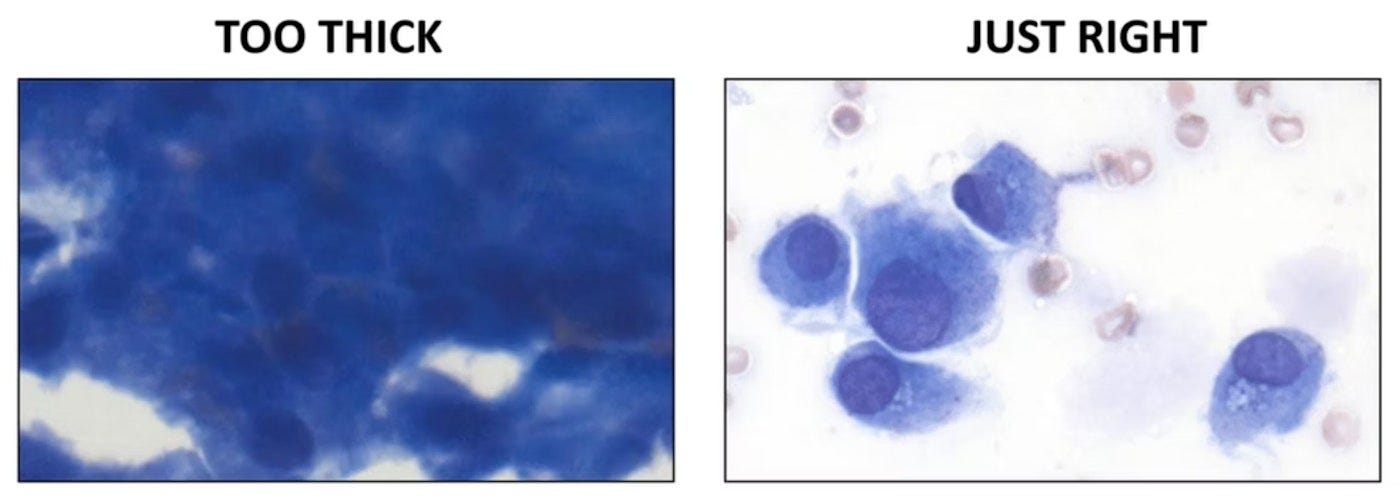
The cells on the left below are too packed to discern any morphologic features, so you wouldn't want to spend much time looking there. This is common in the very middle of the smear (area in dark blue on the diagram). The cells on the right are nicely spread out and we can tell what they are (spindle cells). This is a classic example of a "monolayer" and you'd find this in the light blue and purple zones above.
Here at All Science, we are on the PBS/NPR model: the vast majority of content is FREE, and paid subscriptions allow me to do the research and writing that goes into producing the site, as well as to give back to the community (donations to the Humane Society of Tampa Bay). If you find yourself enjoying these articles, consider becoming a free or paid subscriber 👇
Tip #3: Make sure you’re looking at intact cells
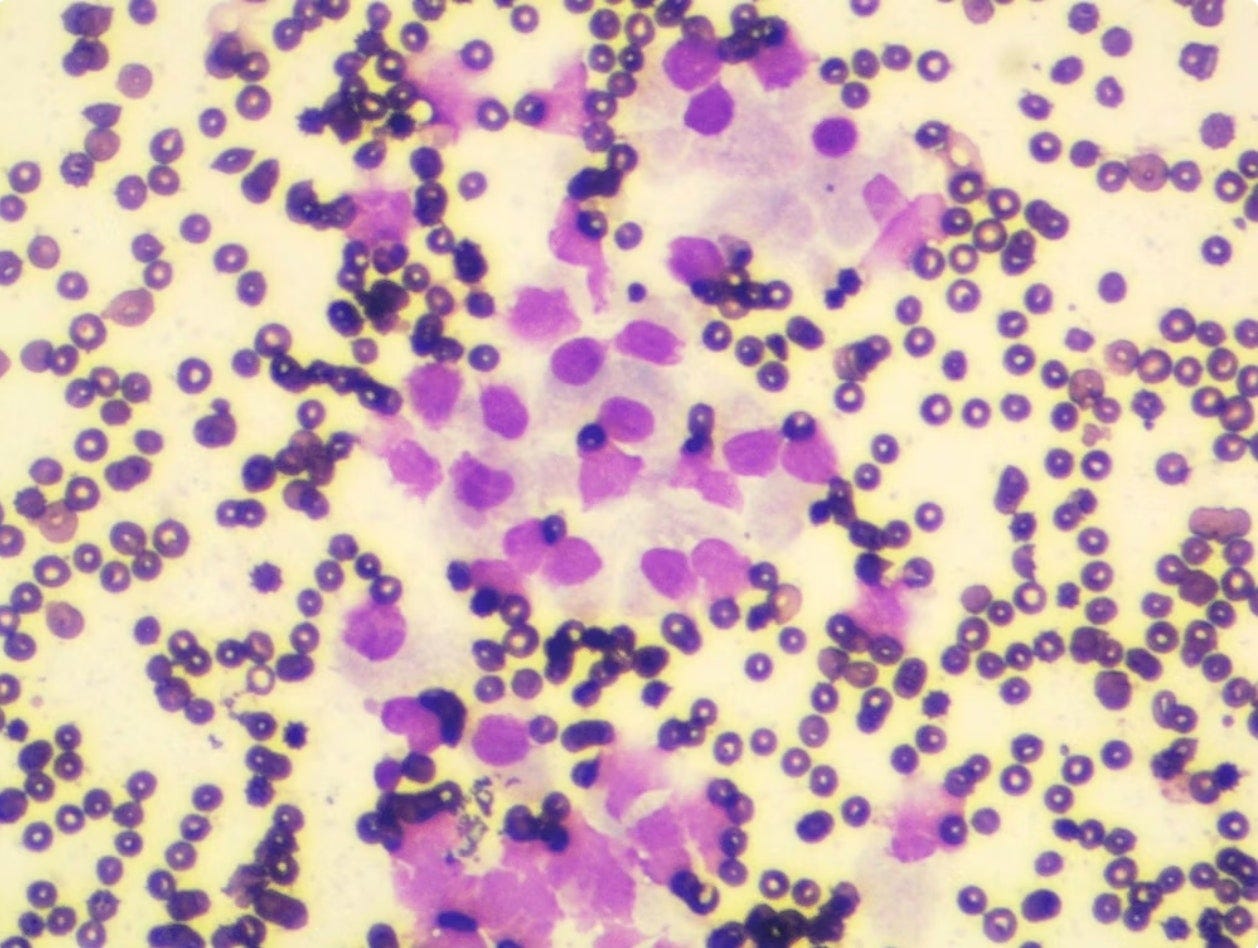
As pathologists, we always feel bad when we have to call things non-diagnostic, but if all or most of the cells we see are look like the examples below, we don’t have any choice 🫤
This image is a classic example of overspread and ruptured cells. The only thing left is smears and puffs of nuclear chromatin. Sometimes people call these "basket cells" or “burst cells” when they're seen on a blood smear. We can't make heads or tails of these, unfortunately. This issue can be found anywhere on a slide, but they're especially present at the edges of the smear (ID’ed in light pink on the diagram above).
While some degree of cellular lysis is expected in all samples, it can be significant in tissues with fragile cells (particularly lymph nodes). General helpful tips that in some cases can help prevent excessive cell lysis include:
Don’t apply negative pressure suction during fine-needle aspiration (woodpecker technique)
Avoid using excessive force on the syringe when expelling the sample onto the slide
Ensure the needle is in direct contact with the slide when expelling the sample (not above the glass)
Most importantly, use only the weight of the glass slide to gently spread the sample (no added hand pressure/downward pressure required).




Remember, when you’re looking at cells on a slide: If you can’t see any borders or cytoplasm around the nucleus, it is probably not intact and should be skipped.
Tip #4: Put the condenser in the right position
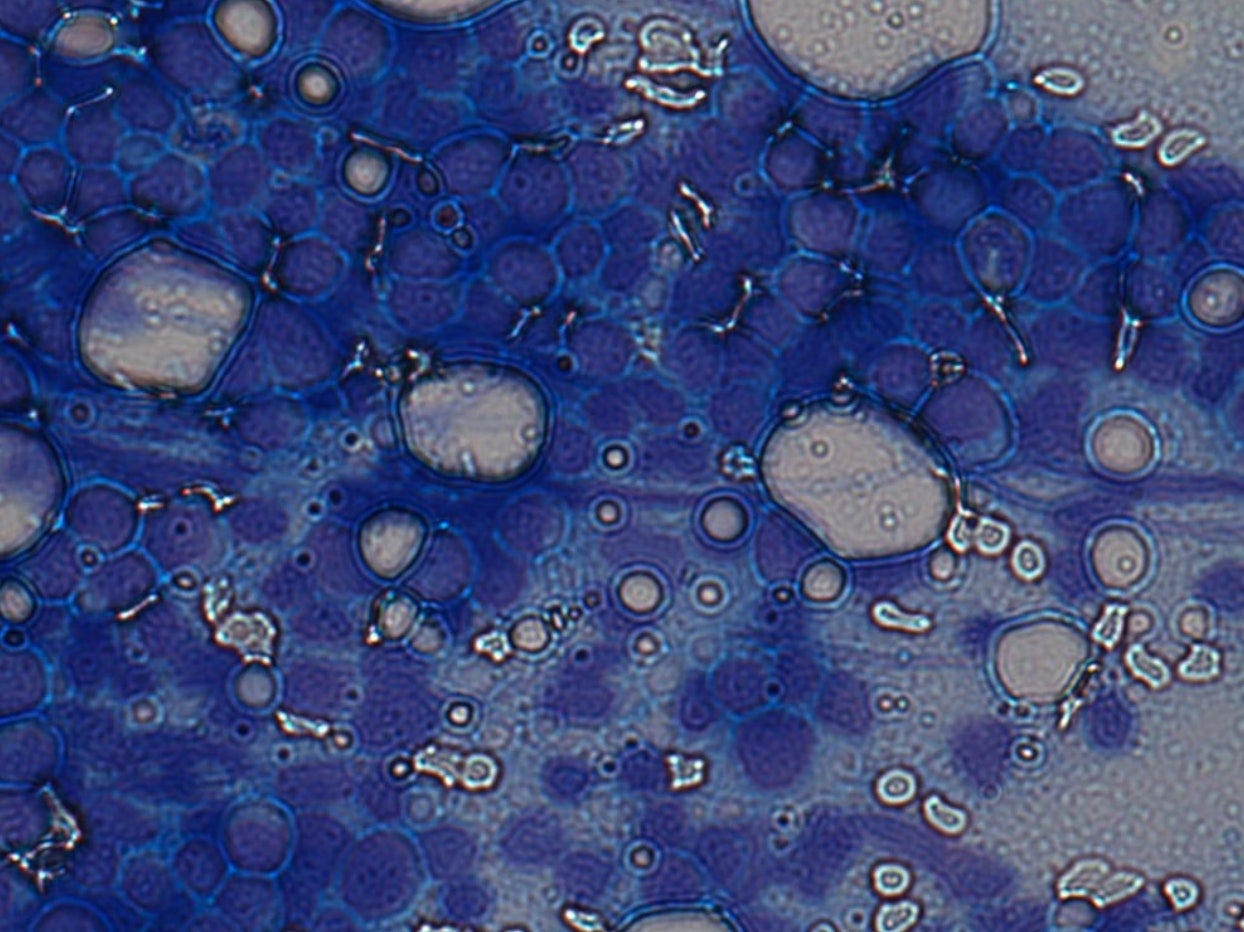
Here's another quick tip: Make sure that when you're reviewing cytology/CBC slides on the microscope you raise the substage condenser to the correct position right below the stage where you place your slide. Lowering the condenser is common for reviewing unstained urine sediment and fecal O+Ps because it increases contrast, and sometimes the last person leaves the microscope stuck in that configuration until you sit down to look at a blood smear or cytology slide.

If you don't move it to the right position, the field of view will look grainy and "refractile," making it hard to interpret. This is an image from a classic case of lymphoma, but with the dropped condenser, everything looks like a 60s moon landing photo and I wouldn't be able to make heads or tails of the sample!
This effect is especially important to be aware of if you are taking photos for digital cytology consults.
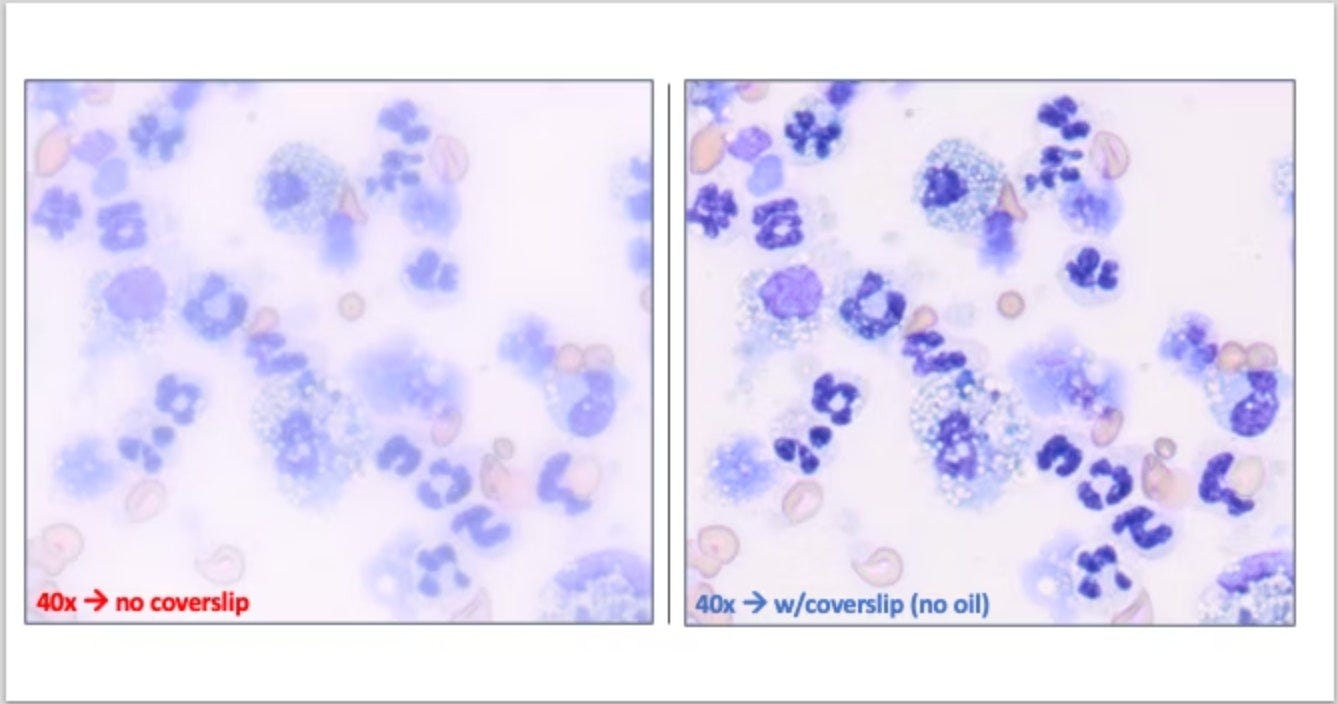
Tip #5: Use a coverslip!
Finally, who here has ever lamented that their 40x lens always seems to be dirty or broken and you can't fix it? When I ask this question to audiences in continuing ed lectures, nearly every hand goes up 🙋🏻♂️
Here's a little secret: Most 40x objectives are made to be used with coverslips, and you actually can't even focus without one!!
This image shows the same exact field at 40x with and without a coverslip....what a dramatic difference! You can place a drop of oil on the slide and then the coverslip on top to help it stick better and further improve focus, but you can get a significant improvement just laying one on the slide "dry."
This trick is especially helpful to let you browse more of the slide faster. One of the most common mistakes I see people make is immediately jumping to 100x oil and spending a lot of time looking in a suboptimal area (see Tip #2). At a mid-high magnification like 40x, you can do a more efficient and thorough review of the slide!
Eric, I'm just joking here, but what would be the harm in adding a semester in med school to nothing but pathology instruction? One could argue that pathology is the queen of diagnosis and accurate diagnosis is at the center of medical practice!
This was a fun post, as I don't have the opportunity to look at slides anymore. Used to do BV swabs and rarely gout aspirations, but the fast pace of primary care has left anything like this in the dust. I'm sure others will find practical benefit from this post, and I enjoyed the science and technique.